- Cigarette smoking
- Family history of heart disease
- Age above 45 years for men and 55 years for women
- Smoking
- High cholesterol
- Diabetes
- High blood pressure
- History of heart attack or known coronary artery disease
- Acute ST-elevation myocardial infarction (STEMI)
- Chest discomfort
- Shortness of breath
- Dizziness
- Fatigue
- Nausea
- Pain in the upper body or arm
- Rapid or irregular heartbeat
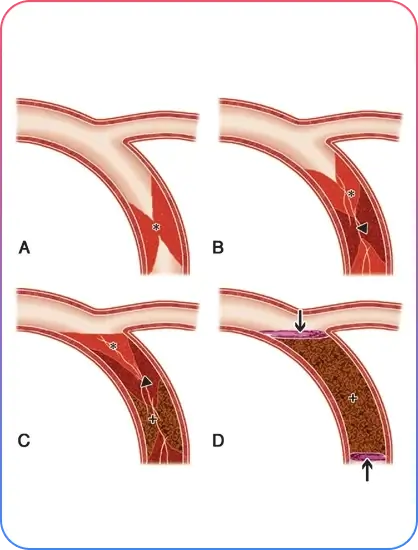
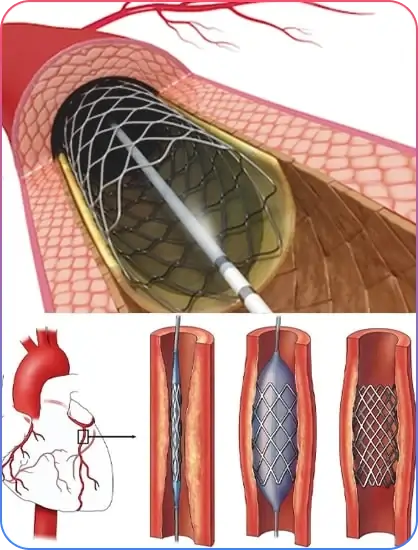
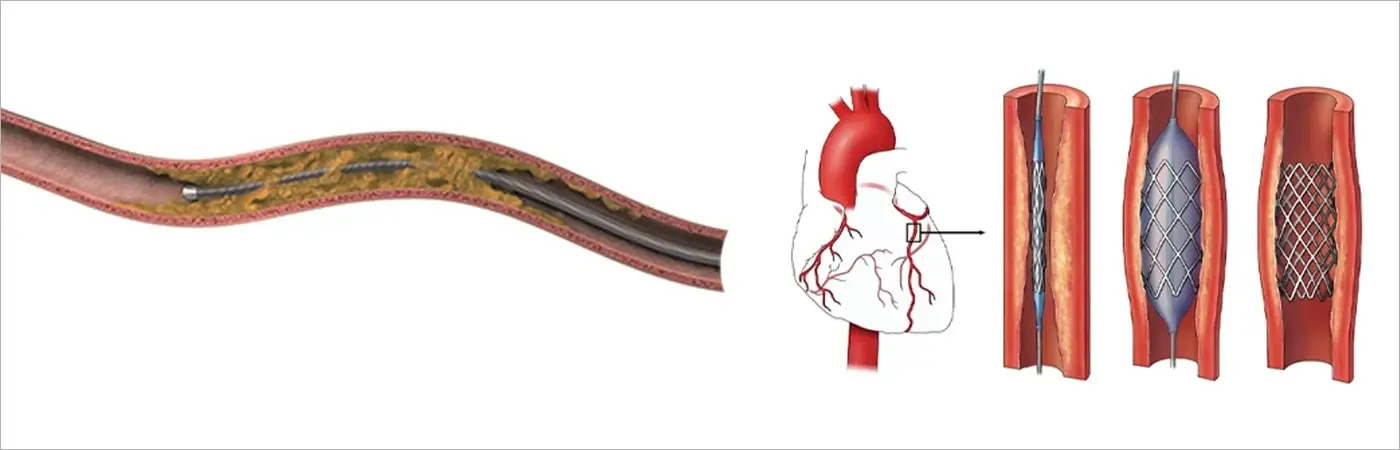
Obstructive Coronary Artery Disease
Diagnosis of CTO is based on:
- Patients’ medical history
- Physical examination: Complete auscultation of the heart and lung sounds together with assessment for heart failure signs including jugular venous distention, Kussmaul sign, hepatojugular reflex, ascites, and peripheral edema.
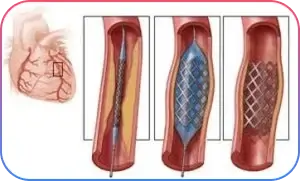
- Coronary angiogram procedure: During this procedure, contrast material is injected into the coronary arteries and pictures are taken to identify blockages and assess heart muscle and valve function.
- EKG
- Echocardiogram (ECG)
- Stress test
- Nuclear medicine PET scan
- Cardiac MRI