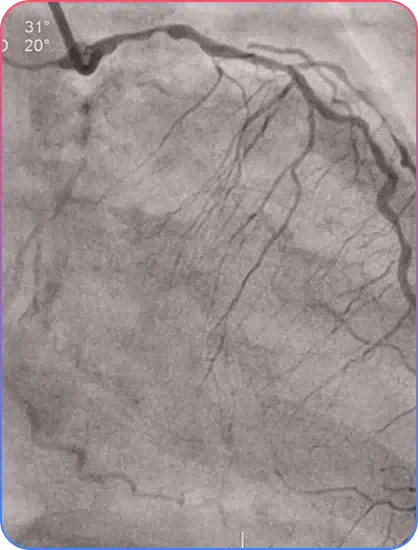
What is a bifurcation blockage?
Stenoses, or narrowing, located in a main coronary artery and an adjoining side-branch vessel.
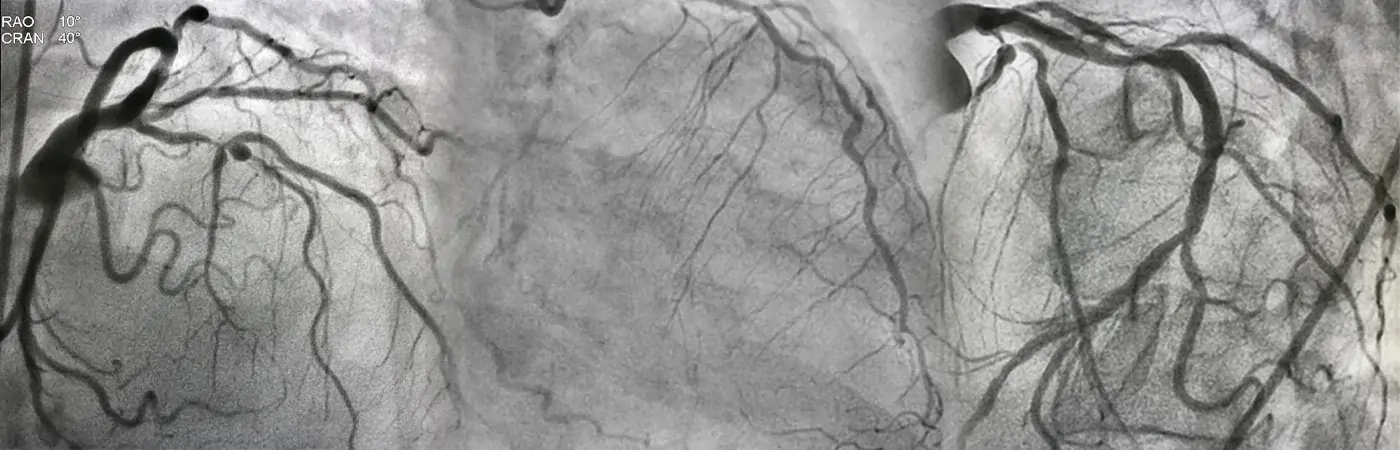
What is a bifurcated stent?
It is a novel platform designed to permit stenting in bifurcation lesions regardless of branch angulation or plaque location, in a short and simple procedure.