Art of Re-entry: Practical Strategies for When Your Antegrade Wire Is Subintimal
Re-entering the true lumen after an antegrade wire has gone subintimal is one of the most challenging parts of chronic total occlusion work. It is equal parts planning, technical skill, and adaptability. This guide walks through practical options, preparation, device use, and troubleshooting to help you choose the right strategy and improve the odds of a successful re-entry.
Table of Contents
- Why re-entry planning matters
- Quick overview: Re-entry options
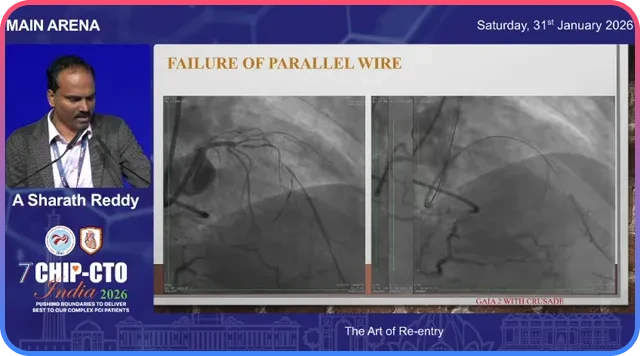
- Common pitfall: Lost vessel clarity after parallel wire or prolonged attempts
- Step 1: Plan re-entry before you lose options
- Tools and techniques
- Case examples and learning points
- Troubleshooting common problems
- Decision checklist before attempting re-entry
- Practical tips from the lab
- Conclusion
Why re-entry planning matters
When a wire enters the subintimal space, your choices narrow quickly. The initial decisions you make — whether to redirect, escalate, use a parallel wire, attempt a dedicated re-entry device, try tip detection with intravascular ultrasound, or go retrograde — shape the anatomy you will be dealing with minutes later.
A key principle: the first three options (redirecting the same wire, escalating the wire, or using a parallel wire with escalation) are mutually exclusive in practical terms. If you stick with one technique for too long, the vessel clarity degrades and other techniques become less likely to work.
Quick overview: Re-entry options
- Redirect same wire — try to recross into true lumen without exchanging or changing position.
- Wire escalation — use stiffer or different polymer wires to penetrate back into true lumen.
- Parallel wire with escalation — create a new channel beside the first wire using a stiffer wire.
- Dedicated re-entry device (Stingray) — intentionally enter subintimal space and use Stingray system to exit into true lumen.
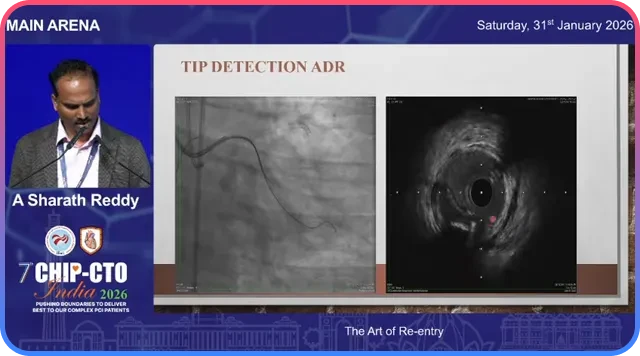
- Tip detection ADR using IVUS (Iris/IVUS-guided) — visualize the vessel from within the subintimal space and guide the wire back into lumen.
- Retrograde approach — approach the CTO from collaterals to facilitate re-entry, sometimes with balloon protection (facilitated ADR).
Common pitfall: Lost vessel clarity after parallel wire or prolonged attempts
When you attempt redirection or parallel wire techniques, repeated manipulation and time cause the vessel clarity to degrade. Contrast tracks obscure the lumen and a growing subintimal hematoma compresses the true lumen. When that happens, even a device like Stingray may have a much lower chance of success.
The practical takeaway is to avoid prolonged trial-and-error with multiple techniques in sequence. Decide early, keep your re-entry zone protected, and switch tactics before the vessel becomes unusable.
Step 1: Plan re-entry before you lose options
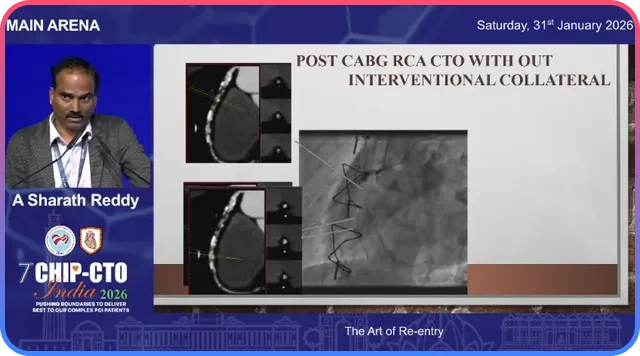
For any case without a reliable interventional collateral, plan your re-entry zone up front. CT angiography is exceptionally helpful for mapping the distal lumen and identifying calcium-free windows suitable for re-entry.
If you anticipate no retrograde options, obtain a CT and choose a re-entry spot you can protect from knuckle tracks and subintimal hematoma.
- Where is the planned site of re-entry?
- What support will you have for device delivery?
- What is your dissection or crossing strategy?
- How will you save your re-entry zone from intramural hematoma?
- What re-entry method will you choose?
Tools and techniques
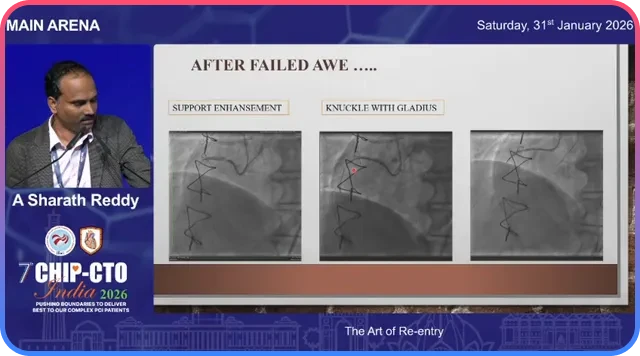
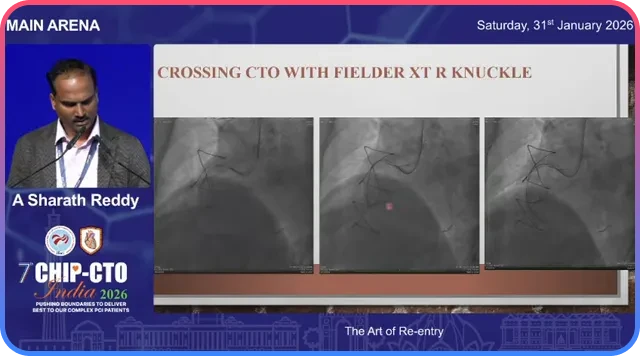
Knuckle and gladius strategy
A sliding “gladius” knuckle is often used to traverse long segments safely in the subintimal plane. Unlike a rolling knuckle, a sliding knuckle moves forward smoothly and can sometimes re-enter the true lumen on its own.
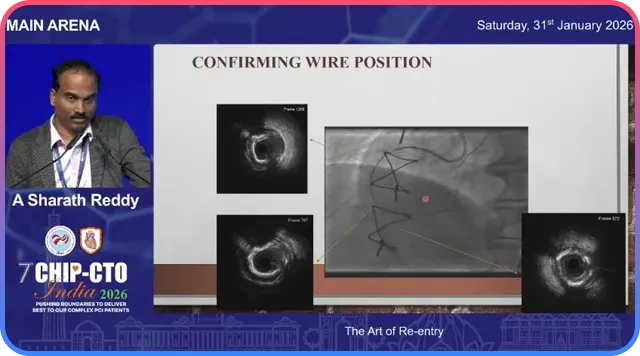
Always confirm position using a workhorse wire into nearby branches to verify entry into true lumen.
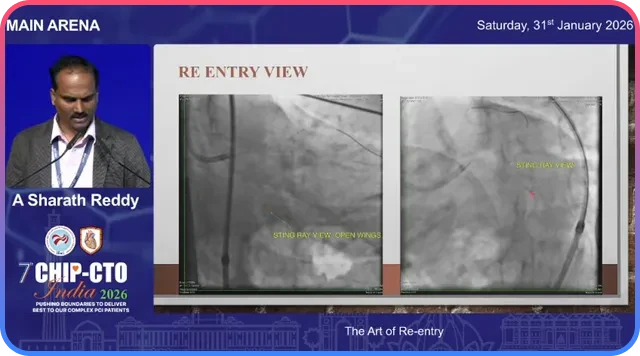
Stingray re-entry device
The Stingray system is the go-to when you intentionally perform antegrade dissection and re-entry (ADR) or when the wire has gone subintimal but you have a clear re-entry territory.
- Choose a visible, non-calcified re-entry zone.
- Enhance support using anchor or support wires.
- Create space using small balloon dilation or microcatheters.
- Use correct imaging orientation for accurate re-entry.
- Swap to a workhorse or Pilot wire after successful lumen access.
IVUS-guided tip detection (Iris catheter)
IVUS-guided tip detection allows direct visualization of the device tip relative to the true lumen and helps position the wire precisely for re-entry.
This is especially useful when the subintimal space is large and the distal vessel morphology remains preserved.
Facilitated ADR with retrograde balloon protection
Facilitated ADR uses a retrograde wire and balloon to protect the true lumen while an antegrade wire is directed toward the balloon for controlled re-entry.
- Advance retrograde wire into distal true lumen.
- Inflate balloon to protect the lumen.
- Direct antegrade wire toward protected target.
Case examples and learning points
Case: Accidental knuckle re-entry
A gladius knuckle unexpectedly re-entered the true lumen. Confirmation came through branch wiring and IVUS imaging.
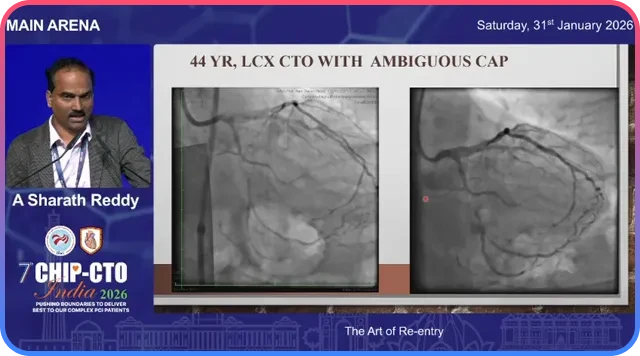
Case: Ambiguous cap LCx CTO managed with Stingray
After entering subintimal space, the operator selected a clear angiographic re-entry zone, advanced Stingray with support, and successfully exited into true lumen.
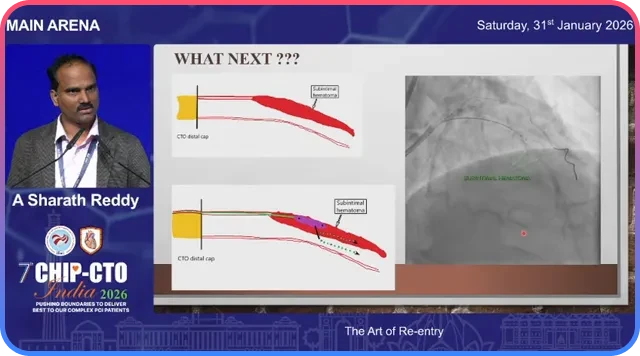
Case: Difficult re-entry with increased subintimal hematoma
Repeated wire attempts created a large subintimal hematoma compressing the true lumen. STRAW maneuvers and Stingray repositioning ultimately enabled successful re-entry.
Troubleshooting common problems
When the swap wire keeps buckling
- Reduce hematoma with STRAW or aspiration.
- Reposition Stingray slightly.
- Consider IVUS-guided tip detection.
When vessel is heavily calcified
Use CT to identify calcium-free windows. If none exist, consider retrograde or hybrid strategies.
No interventional collateral and failed re-entry
An investment strategy with staged intervention may preserve distal perfusion and facilitate future reattempts.
Decision checklist before attempting re-entry
- Is there an interventional collateral?
- Is the selected re-entry zone free of heavy calcium?
- Can support be enhanced for device delivery?
- Are all required devices available?
- Is there a plan to reduce hematoma?
- What is the bailout strategy if re-entry fails?
Practical tips from the lab
- Protect your planned re-entry zone.
- Use small balloon dilation for Stingray preparation.
- Recognize proper Stingray imaging views.
- Switch strategies early if one approach fails.
- Use facilitated ADR when safe retrograde access exists.
- Use IVUS for tip detection and procedural planning.
Conclusion
Re-entry is an art informed by planning, imaging, and timely strategy selection. Protecting the re-entry zone, using the right devices, and switching tactics early are essential for procedural success.
When anatomy becomes hostile with large hematomas or poor re-entry windows, an investment and staged approach may be safer than aggressive high-risk attempts.
Frequently Asked Questions
It means the guidewire has left the true lumen and entered the subintimal (false lumen) space between the intima and media during CTO intervention.
No. It may be accidental or intentional as part of ADR (Antegrade Dissection and Re-entry). Controlled subintimal navigation is common in modern CTO practice.
Options include redirecting the same wire, wire escalation, parallel wire technique, Stingray re-entry device, or retrograde access.
Parallel wire works best when vessel clarity is preserved and hematoma is minimal. Stingray is preferred for controlled ADR with a visible re-entry zone.
Waiting too long to switch strategies. Repeated manipulation increases hematoma and reduces vessel clarity.
Signs include wire buckling, inability to wire side branches, resistance during advancement, and lack of distal filling.
STRAW maneuvers, aspiration, decompression, IVUS-guided targeting, and repositioning the re-entry zone can reduce hematoma.
IVUS is useful when angiographic cues are unclear, subintimal space is large, or Stingray attempts are inconclusive.
Facilitated ADR combines retrograde balloon protection with antegrade re-entry and is useful in post-CABG or complex distal vessel cases.
Not always. Retrograde strategy depends on collateral quality, operator expertise, patient stability, and procedural risk.
It involves creating a controlled subintimal channel, preserving distal perfusion, and staging definitive treatment later.
CT angiography helps identify calcium-free re-entry zones, distal vessel anatomy, and procedural difficulty.
Common wires include Gaia 2, Gaia 3, Pilot series, workhorse wires, and dedicated Stingray wires.
Pre-identify the zone, avoid large knuckles through it, limit prolonged manipulation, and enhance support early.
Proper en-face orientation and contrast injection through the Stingray balloon are critical for successful re-entry.
Stop when distal vessel compromise, expanding hematoma, unsafe contrast load, or excessive radiation risk outweighs benefit.
Decide early, switch early, and protect the distal vessel.
Yes. A sliding knuckle may occasionally re-enter spontaneously, but true lumen position must always be confirmed.
Heavy calcification reduces Stingray success and may require CT planning, IVUS guidance, or retrograde strategies.
Experts plan early, preserve vessel clarity, use imaging extensively, switch techniques decisively, and accept staging when necessary.