




Dr. Sharath Reddy
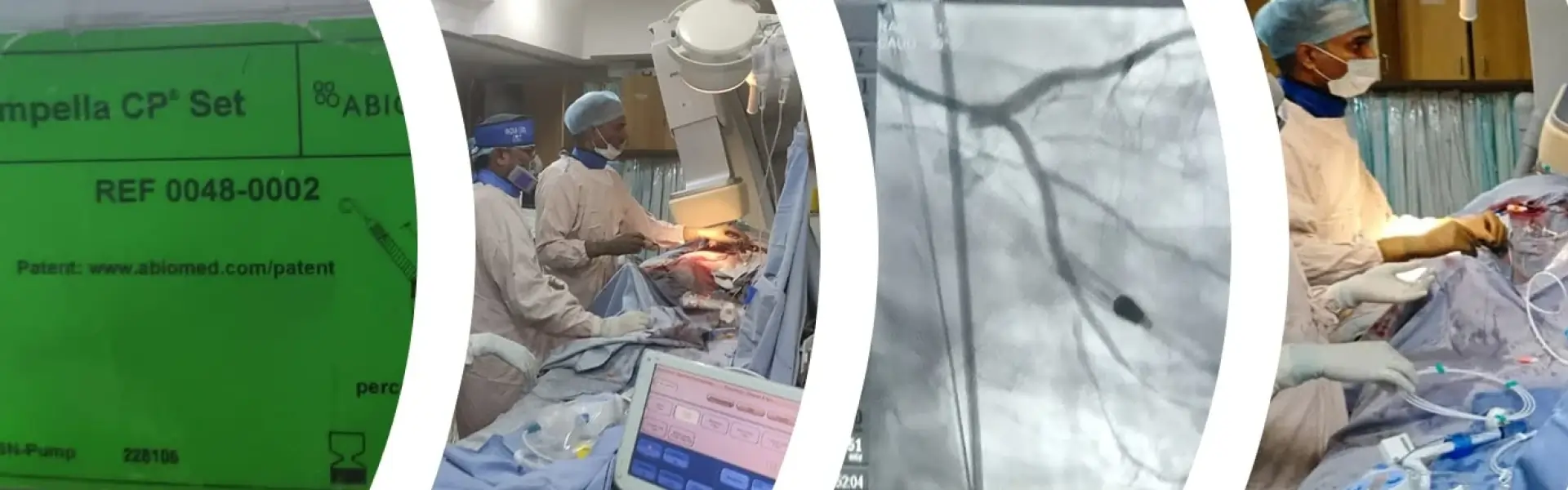
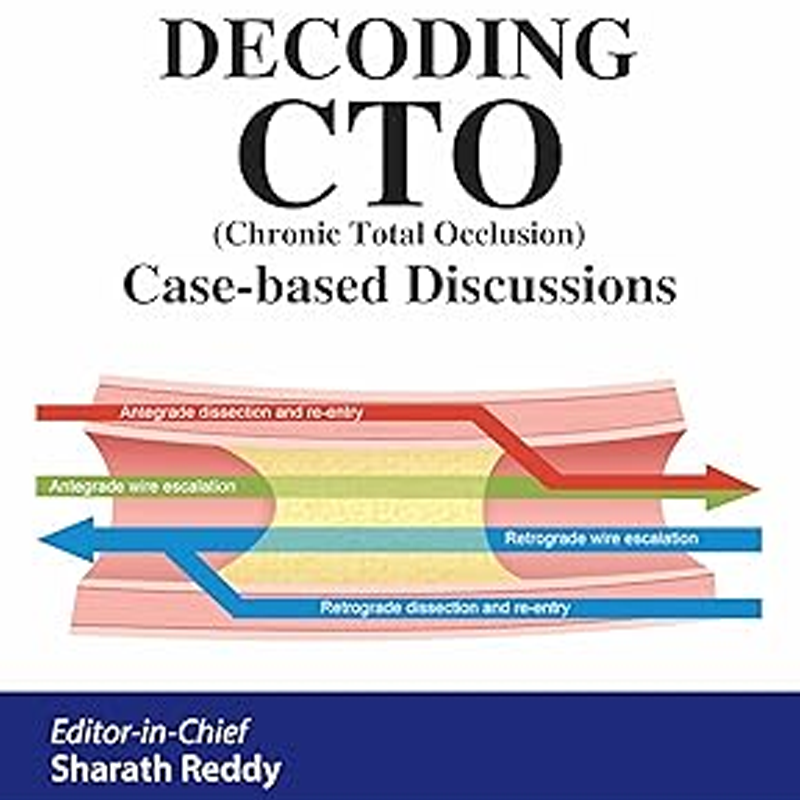
Dr. Sharath Reddy A is one of the few to be ranked in the league of eminent cardiologists. With an unparalleled track record, he is presently the Founder-Director of Medicover Hospitals and the Director of Cath Lab at Medicover Hospitals, Hitec City, specializing in interventional cardiology. He is a Proctor for complex coronary interventions, imaging-guided interventions (specifically Intravascular Ultrasound), interventions with rotablation, and chronic total occlusion (CTO) percutaneous coronary interventions (Antegrade, Retrograde, and Antegrade Dissection and Re-entry). He is one of the most sought-after interventional cardiologists for heart valve disease treatments, such as Transcatheter Aortic Valve Replacement/Implantation (TAVR/TAVI) and Percutaneous Balloon Mitral Valvuloplasty (PBMV).
About Doctor
By the numbers: excellence in health
8000+
Coronary Angiographies
5000+
Coronary Angioplasties
500+
CTO Procedures
1000+
Structural Heart Procedures
17
Peer-Reviewed Publications
500+
Workshops as Speaker / Proctor
Empowering Hearts Through Service, Knowledge, and Innovation


19+ Years
Advanced Cardiac Expertise
Evidence-based Treatment
Personalized cardiac care with modern medical standards.
Top-notch Experience
Trusted expertise in advanced heart procedures.
Quality Care
Compassionate patient-focused treatment approach.
Advanced Technologies
State-of-the-art cardiac diagnostics and interventions.
WHERE PEOPLE COME FIRST

95%
Success rate with coronary interventions

TAVR
Advanced planning & execution expertise

Global
Proctor across Asia & India

Pioneer
Early adopter of TAVR procedures
Field of Specialization
- CTO PCI
- COMPLEX ANGIOPLASTIES
- CHIP-PCI
- FAILED ANGIOPLASTY TREATMENT
- POST-CABG BLOCKAGE TREATMENT
- LEVEL-1 CARDIAC EMERGENCY CARE
- TAVR / TAVI
- PBMV
- IMAGING-GUIDED INTERVENTIONS
- ROTABLATION FFR
- CORONARY ANGIOGRAM
- CT CORONARY ANGIOGRAM

Advanced Cardiac Care
Complex Interventions & Structural Procedures