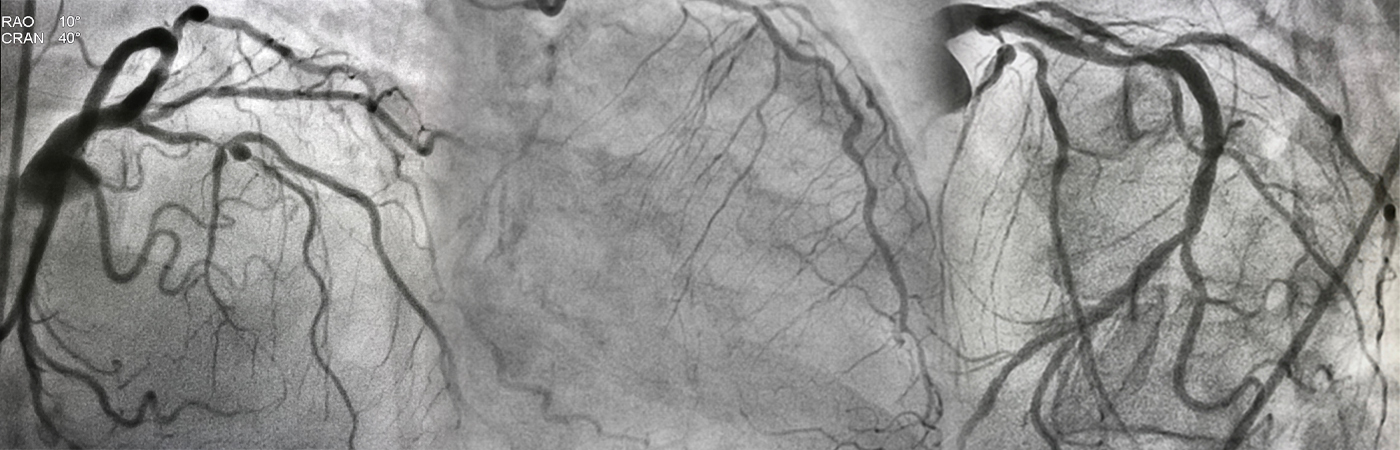
Bifurcation
Bifurcation Lesion is a coronary artery narrowing occurring adjacent to, and/or involving, the origin of a significant side branch that you do not want to lose.
In simple terms, it is a lesion in parent vessel very close or involving a significant side branch.
Drug-eluting stents (DES) should be used for the treatment of bifurcation lesions, as treatment with bare metal stents (BMS) ha yield sub-optimal results.


Bifurcation
Blockage
What is a bifurcation blockage?
Bifurcated
Stent
What is a bifurcated stent?
The left main is the largest bifurcation of the coronary tree and is, therefore, easier to access.
Types of
Left Main
Bifurcation
One-Stent Approach with Provisional Side Branch Stenting
- Wire both the Main Branch(MB) and Side Branch(SB) with coronary guidewires. Predilate the Main Branch.
- Main branch stenting sized to the distal main branch reference diameter with jailing of the SB wire.
- Assessment of the angiographic result in the MB and SB.
- Attempt to rewire the SB through the distal MB stent strut to enhance SB scaffolding. (If successful, remove the jailed SB wire.)
- After the SB is rewired, dilate the SB.
- Assessment of the angiographic result in the MB and SB.
- If the SB result is suboptimal, perform final kissing inflation (FKI) or preferably sequential side-main-side (SMS) balloon dilatation on the SB and MB with a noncompliant balloon or assess the hemodynamic significance of the SB with fractional flow reserve (FFR).
- SB stenting if the SB in ≥2.5 mm and has ≥75% stenosis, FFR ≤ 0.80, TIMI (thrombolysis in myocardial infarction) flow grade < 3, or plaque shift into the SB.
- After SB stenting, repeat FKI or SMS.


Two-Stent Approach
- Classic T-stent and Modified T-stent Technique
- TAP Technique– This technique is typically used with the provisional one-stent approach; however, it can also be used for the elective two-stent approach.
- Culotte Technique-allowscoverage for complete lesion. It should preferably be performed with stent platforms that have an open cell design.
- Mini-crush and Step-crush technique– The mini-crush technique has replaced the original technique by reducing the number of overlapping stents in the proximal MB. In the step-crush technique, the main difference is that the protruded SB stent is “crushed” with a noncompliant MB balloon.
- V- stent and SKS Techniques – Both techniques employ simultaneous implantation of the MB and SB stents, difference between the two techniques is the amount of stent protrusion into the proximal MB. A small amount is V-stent technique, whereas a significant amount is the simultaneous kissing stent (SKS) technique.
"Dr. Sharath Reddy is the best cardiologist in Hyderabad. We underwent the heart treatment under him. We are very happy with the treatment."
I would like to thank Dr Sharath Reddy and his team for the excellent cardiac care and treatment provided to me. I have been given all the information and advice to lead my life in a comfortable way after the procedure. I can’t thank you enough for all your time, hard work, and patience. I truly appreciate your caring dedication.
My brother had severe dyspnoea (shortness of breath) and it was difficult for him to walk for even very small distances. He had severe pedal oedema (feet swelling) and was not able to do routine activities on his own. But after TAVI procedure he is able to breathe well and walk comfortably for small distances without any difficulty. Within a short time after the TAVI procedure he is performing his routine own activities. We are grateful to the cardiac team at Medicover Hospitals.
