Art of Cannulating Coronary Arteries while doing Angiogram
Cannulating coronary arteries is a fundamental skill in interventional cardiology. Precision, patience, and small technical adjustments often make the difference between a smooth, safe angiogram and a difficult or potentially traumatic attempt. This guide collects practical tips and tactical maneuvers for engaging the left and right coronary systems reliably, avoiding common pitfalls, and protecting the coronary ostium during both diagnostic angiography and angioplasty.
Why technique matters
Every coronary anatomy is unique. Standard catheters and routine maneuvers work most of the time, but anomalies and subtle positional differences of the ostium demand deliberate variations in approach.
The priorities during cannulation are:
- Safety: avoid forceful pushing that can injure the ostium.
- Visualization: choose the projection that best reveals the sinus and ostium.
- Coaxiality: obtain alignment so contrast injections are safe and diagnostic.
- Readiness: verify pressure traces and have a wire ready before selective injections.
Checklist before any injection
- Confirm catheter tip location in the aortic sinus by gentle pullback and visual cues.
- Observe the pressure waveform; never inject contrast if waveform suggests damping or occlusion.
- Keep a guidewire ready when anatomy or coaxiality is uncertain.
- Choose the ideal angiographic projection before manipulating the catheter.
Left Coronary Cannulation: Step-by-Step Maneuvers

1. Standard Approach
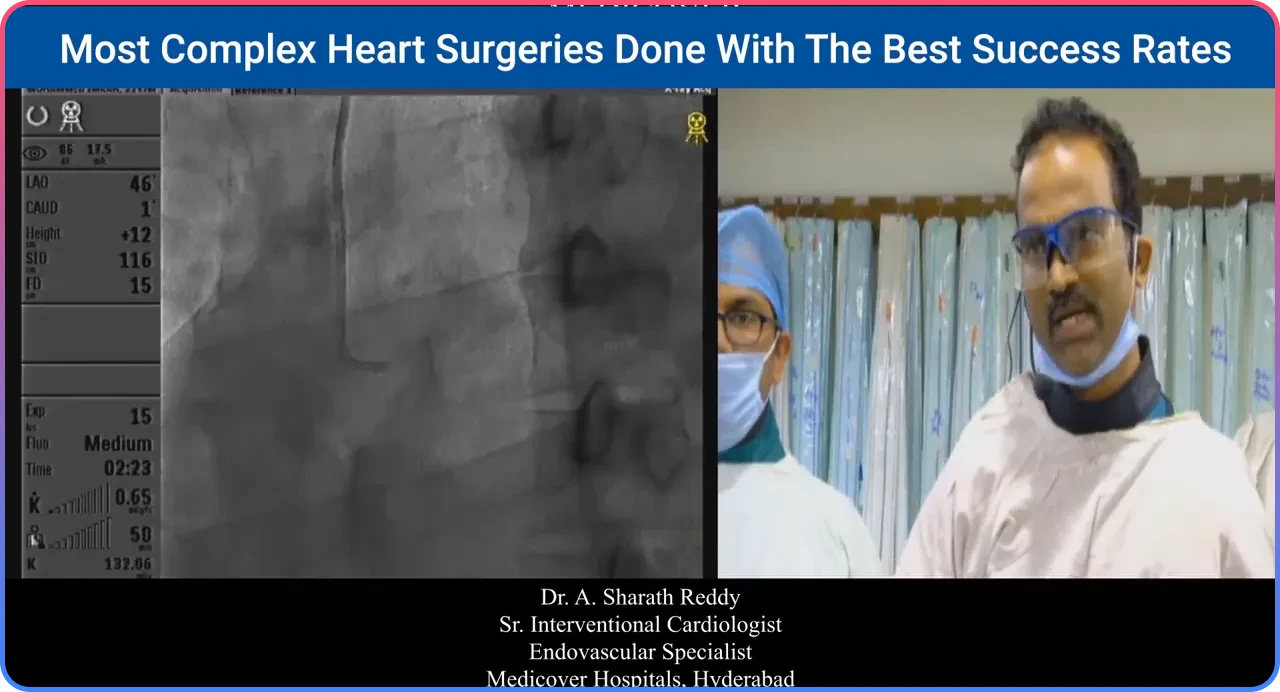
With the diagnostic catheter parked in the left coronary sinus, gently pull back while watching the catheter tip. When the tip begins moving with the ostial rhythm and the pressure waveform is preserved, selective engagement is usually achieved.
2. Deep-Breath Maneuver
If engagement fails in the standard view, ask the patient for a deep breath while the catheter remains in the left sinus. Deep inspiration often changes the aorto-coronary geometry enough to allow engagement with gentle downward pressure.
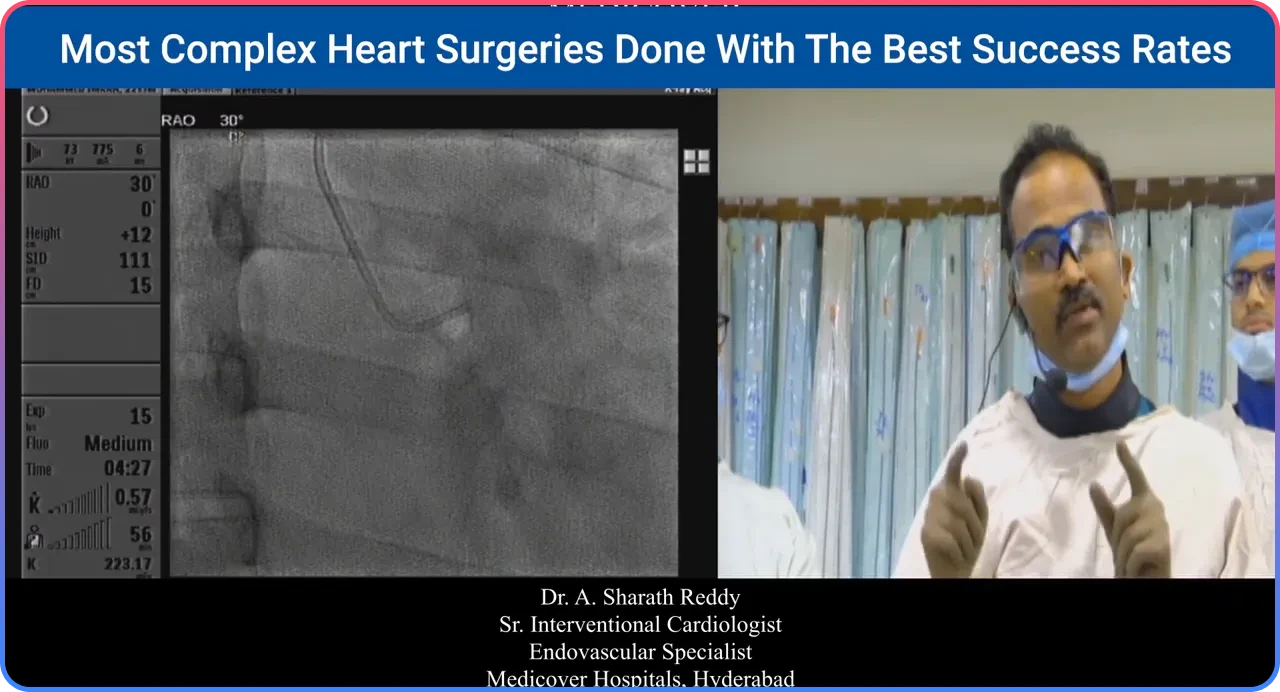
3. Use an End-On or RAO View
When the ostium appears displaced posteriorly, switch to a right anterior oblique (RAO) projection. A small non-selective injection in RAO can outline the sinus and identify whether the LMCA origin is central or posterior.
- Clockwise rotation: Directs the catheter tip anteriorly.
- Anti-clockwise rotation: Directs the catheter tip posteriorly.
4. Avoid Forceful Pushing
Aggressive pushing may traumatize the coronary ostium. Projection-based localization, precise rotation, and gentle movements are safer and more effective.
5. Make the Guide Coaxial with a Wire
When the catheter is engaged but not fully coaxial, advance a wire across the ostium. The wire stabilizes alignment and reduces the risk of trauma during injection.
Common Left-Side Problems and Solutions
Catheter Entering the Left Circumflex in a Short Left Main
In short left main anatomy, the catheter may preferentially enter the LCX. To correct this:
- Move to the LAO cranial or level projection.
- Rotate the catheter slightly anti-clockwise.
- Withdraw marginally and apply a gentle push.
- Reorient the tip toward the LAD for better engagement.
Right Coronary Cannulation: Practical Tips
1. Standard Clockwise Rotation
Rotate the catheter clockwise to align with a mid-sinus RCA origin. Confirm engagement by checking the pressure waveform before injecting.
2. Catheter Tracking into the Conus
If the catheter repeatedly enters the conus or pressure damping occurs, pull the catheter slightly downward and rotate anti-clockwise to realign with the RCA ostium.
3. Back-End Wire Technique
Insert the blunt back end of an 0.035 wire into the catheter to neutralize the secondary curve. This straightens the catheter tip and helps engage a low RCA origin more safely.
4. RCA Originating Anteriorly or Anomalously
For anterior or anomalous RCA origins:
- Rotate clockwise to move the tip anteriorly.
- Switch to RAO projection to assess orientation.
- Perform a small non-selective injection to locate the ostium.

5. When selective engagement fails: three non-selective sinus injections
If you cannot selectively cannulate the RCA despite the maneuvers above, perform systematic non-selective injections in three positions to localize an anomalous origin:
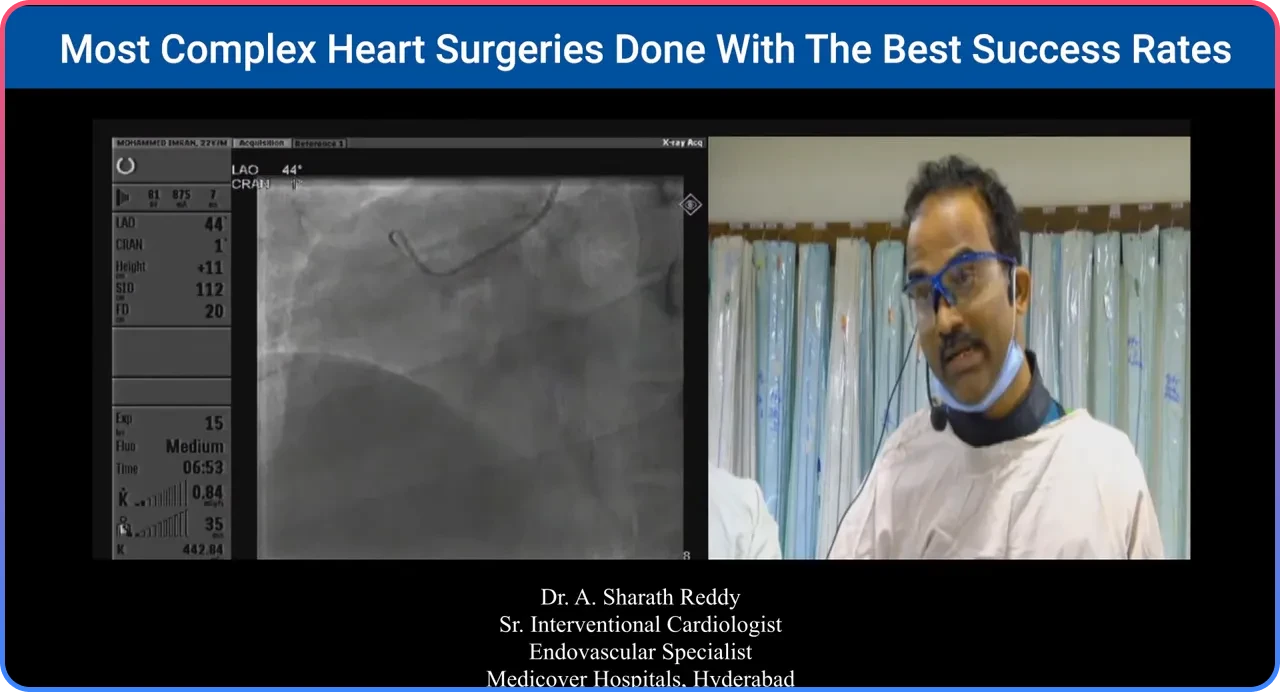
- LAO with the catheter tip facing left of the panel.Inject to visualize the leftward sinus.
- RAO with the tip anterior in the right sinus.Inject to reveal an anterior RCA origin.
- LAO low projection with the catheter in the left sinus (tip anterior).Inject to look for an anomalous RCA arising from the left coronary sinus.
Once the ostium is identified non-selectively, choose a specific catheter shape tailored to the anomalous origin for safe selective cannulation.
Pitfalls, safety tips, and best practices
Small adjustments win. Pushing harder is rarely the best answer. Keep these rules in mind:
- Always check the pressure waveform
before injecting. Damped pressure indicates partial occlusion and high risk for traumatic injection. - Keep a wire handy
during challenging cannulations. Advancing a wire after gentle engagement improves coaxiality and safety. - Prefer projection-based localization
over blind forceful advancement. RAO end-on views show the sinus from posterior to anterior and guide rotation decisions. - Neutralize secondary curves
when necessary with the back end of a wire to change catheter tip orientation safely. - Avoid repeated forceful injections
into a non-coaxial catheter. This can cause coronary dissection or ostial injury.
Quick decision flow for difficult cannulation
- Confirm catheter position and pressure waveform.
- Attempt simple pullback and gentle advancement.
- Ask the patient for a deep breath if needed.
- Switch to RAO end-on view for sinus localization.
- Rotate clockwise or anti-clockwise based on ostial location.
- Advance a guidewire if coaxiality remains poor.
- Use alternate catheter shapes when anatomy is anomalous.
Tools and catheter selection—practical notes
Diagnostic catheters like Tiger or Judkins shapes are the workhorses. During angioplasty, guide catheters with better support are used, but the principles remain the same: localize the ostium first, achieve coaxiality, and avoid traumatic maneuvers.
If an anomalous origin is confirmed, choose a catheter with a primary/secondary curve combination that matches the ostial orientation. When in doubt, non-selective sinus injections in targeted projections are the clue to the correct catheter choice.
Common scenarios and how to approach them
Scenario: Large LMCA, easy cannulation
When the LMCA is large and centrally located, routine technique works reliably. Pullback, check pressure, selective injection, and complete the diagnostic series of projections for the left system.
Scenario: Short left main with catheter tracking into LCX
Use LAO cranial or level views to assess alignment and adjust rotation as described earlier. Slight withdrawal and anti-clockwise rotation will often disengage the LCX and align the tip toward the LAD.
Scenario: RCA origin very low in sinus
The back-end wire trick is especially helpful here. Straightening the secondary curve lets the catheter tip face downward so it can drop into the low RCA ostium without aggressive manipulation.
Final thoughts
Mastery of cannulation is about pattern recognition and incremental adjustments. Use projection strategy to reveal anatomy, rotate deliberately to align the tip, respect the pressure trace, and employ a wire early to make the system coaxial. These small habits reduce complications and speed up diagnostic and interventional procedures.
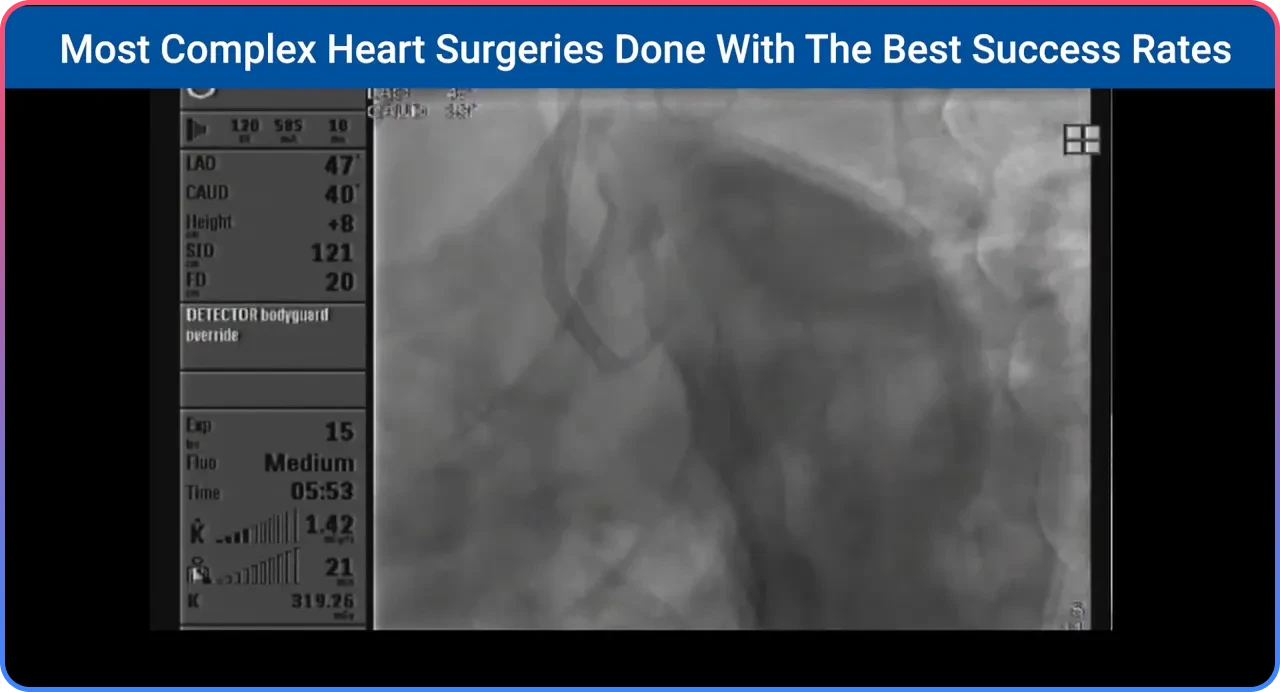
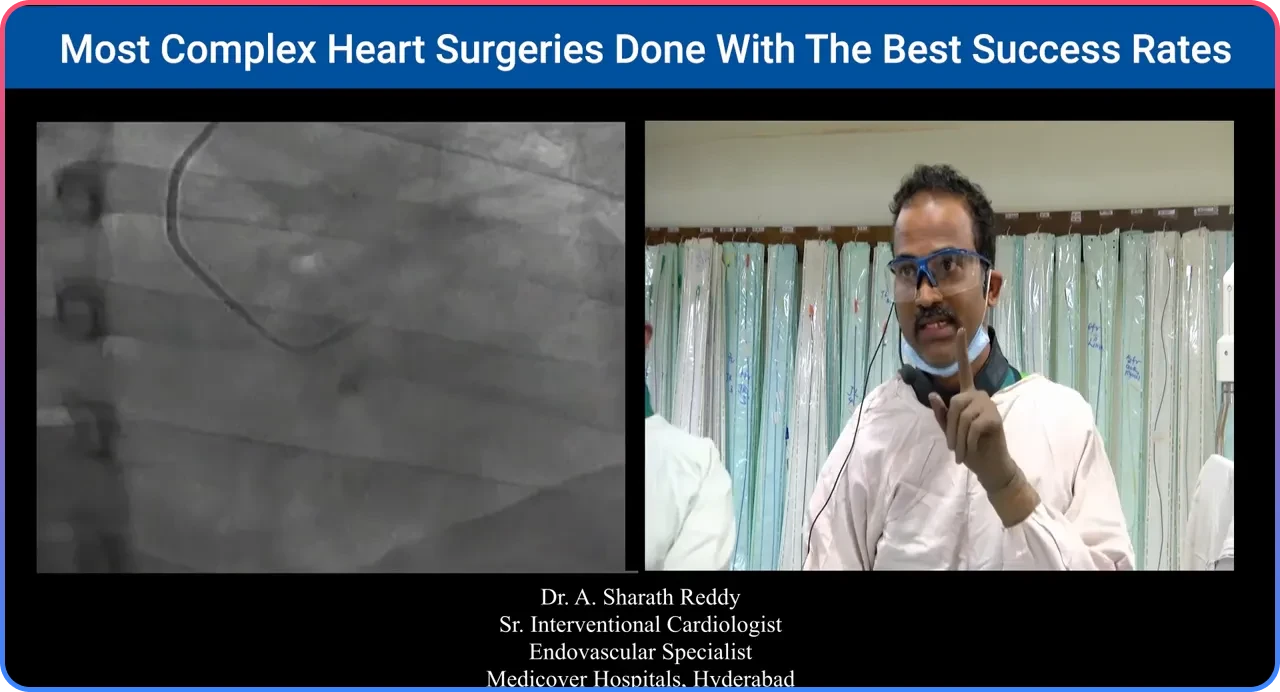
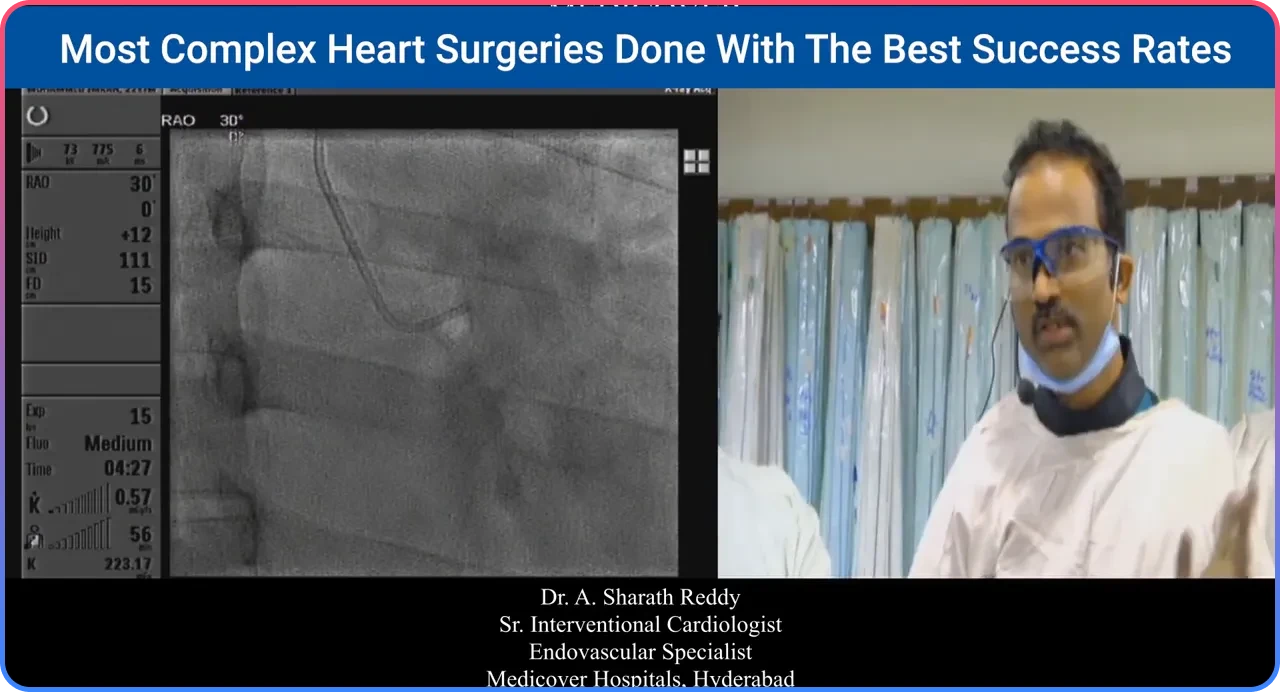
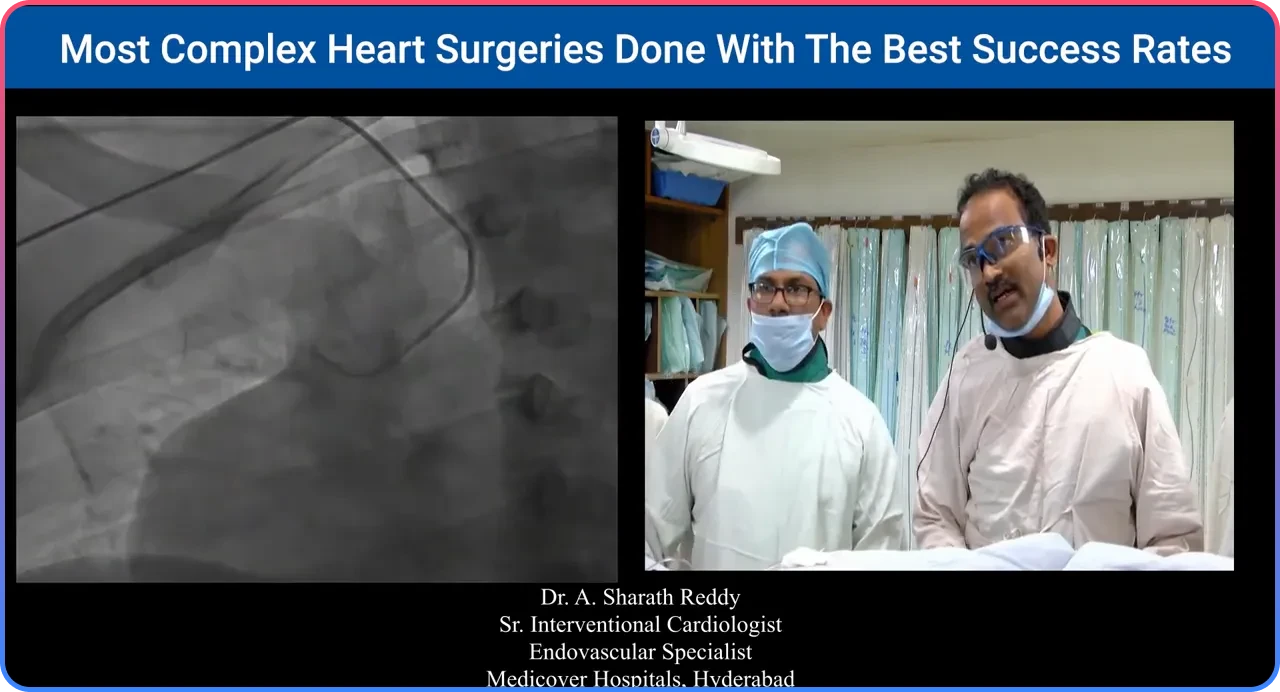
Selected visual references
The images above correspond to key moments during cannulation: catheter parked in the left sinus, RAO end-on sinus injection, rotation maneuvers, back-end wire neutralization, and non-selective sinus injection strategies for anomalous coronaries.

Frequently Asked Questions
Use an RAO end-on projection to visualize the entire coronary sinus. Clockwise rotation generally moves the tip anteriorly, while anti-clockwise rotation directs it posteriorly.
Switch to an LAO level or cranial projection, withdraw slightly, rotate anti-clockwise, and apply a gentle push to redirect the catheter toward the LAD.
No. Aggressive pushing can injure the coronary ostium. Projection-guided positioning and gentle adjustments are much safer.
Use the back-end wire technique when the RCA origin is low or when the catheter repeatedly points toward the conus instead of the RCA ostium.
Perform non-selective injections in multiple projections to identify the anomalous origin and then select a catheter shape that matches the anatomy.